
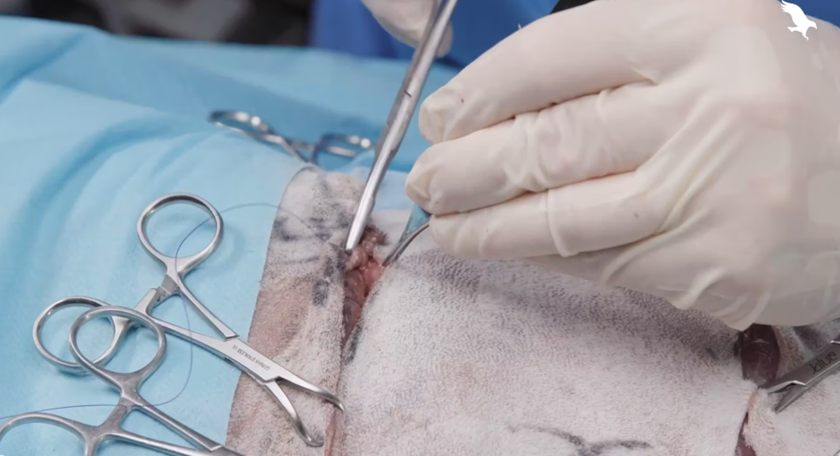
Rotation flaps are an advanced wound closure technique that allows large wounds to be closed without distorting adjacent structures. This step-by-step video shows a rotation flap being created over a wound on the greater trochanter. It was created by Jon Hall MRCVS, RCVS Specialist in Small Animal Surgery.
When to use a rotation flap
Rotation flaps should be considered in small animal surgery when:
- Primary closure would be too tight, causing wound dehiscence, or would distort neighbouring structures
- There is healthy adjacent skin for the donor site
- There is a clean, healthy recipient bed free of debris and necrotic tissue - for traumatic wounds (those not created by surgery), you may have to treat as an open wound until the recipient bed is healthy
- The defect is triangular
How to perform a rotation flap
This video shows the process of creating a rotation flap in small animal surgery.
1. Preparing the patient
The patient should be under general anaesthetic, clipped, prepped, and draped. Ensure the clipped and prepared area is sufficiently wide to allow full development of the curved flap - rotation flaps often require a larger surgical field than initially anticipated, and inadequate preparation may limit flap design or compromise sterility.
2. Preparing the donor site
Assess the shape of the wound. Rotation flaps are best suited to triangular defects or wounds that can be converted into a triangular shape.
With a sterile surgical marker, outline a curved, semicircular flap adjacent to one side of the defect. The flap should originate from the side with the greatest skin laxity. The length of the curving incision should be generous (typically four times the width of the defect, but as long as necessary) to allow the flap to rotate without excessive tension. If in doubt, the arc can be extended during surgery to improve mobility.
The base of the flap should be broad (at least equal to the width of the flap) to preserve blood supply. Avoid designing narrow pedicles, as this increases the risk of flap necrosis.
Incise along the marked curved line and elevate the flap by undermining at the level deep to the panniculus muscle (or just superficial to the underlying fascia where the panniculus is absent), taking care to preserve the subdermal plexus. Handle tissues gently and avoid excessive thinning of the flap.
A backcut may be necessary to allow more movement - make sure this doesn't compromise the flap viability.
3. Placing and fixing the flap
Gently rotate the flap into the defect using stay sutures to assess reach and tension. The flap should sit comfortably without excessive force; if tension is present, further extend the arc of the flap or undermine the surrounding skin to improve mobility.
Once adequate positioning is achieved, begin closure at the point of rotation (the base of the flap) and work towards the distal end. Close the flap into the recipient site in a tension-free manner, taking care not to place excessive sutures that could compromise perfusion.
The secondary defect created by flap rotation can usually be closed primarily, though some undermining may be required. It's usually best to leave any 'dog ears' in place - they typically resolve on their own, and removing them can compromise the flap viability.
Top tips for rotation flaps:
- Gentle tissue handling is essential. Use stay sutures to position and move the flap rather than forceps where possible, reducing the risk of crush injury to the flap margins.
- When elevating the flap, include the subcutaneous tissues to preserve the subdermal plexus. Excessive thinning of the flap will compromise its blood supply and increase the risk of necrosis.
- Avoid electrocautery when incising the flap, as thermal damage can reduce perfusion and affect flap viability.
- Postoperative planning is as important as surgical technique. Consider the need for drains, appropriate bandaging, prevention of self-trauma, adequate analgesia, and clear aftercare instructions.
_BL_CourseThumb.jpg?width=500&height=300&name=IVE_GPCert(STS)_BL_CourseThumb.jpg)
Small Animal Soft Tissue Surgery
ISVPS General Practitioner Certificate (GPCert)
Postgraduate Certificate (PgC)
 April 2026
April 2026
 Online | Swindon
Online | Swindon
Author






