

Brachycephalic obstructive airway syndrome (BOAS) is an increasingly common condition facing general practitioners due to the rising popularity of brachycephalic breeds. Research has improved the recognition and treatment of this disease with the most recent studies providing valuable techniques for grading the severity of disease and accurate data to measure the outcome following individually tailored surgical treatment. Primary conformational abnormalities (stenotic nares, aberrant nasal turbinates, overlong soft palate, narrowed trachea/bronchi) are often exacerbated by secondary airway inflammation or collapse (thickening of the palate, laryngeal collapse).
Diagnosis and grading
Recording a combination of owner and veterinary observations across four major categories can help to organise a complete history: breathing noise, breathing effort, ability to exercise and gastrointestinal signs. Clinical signs of BOAS can include any, or all, of low-pitched pharyngeal noise (stertor), high-pitched laryngeal noise (stridor), increased respiratory effort, exercise intolerance, heat intolerance, sleep apnoea, regurgitation, cyanosis and collapse. While regurgitation can be caused by other conditions (eg food allergies, sliding hiatal hernia, oesophageal dysmotility), it can be the main clinical sign of BOAS in some dogs and in many cases a problem that exacerbates respiratory signs.
Airflow
Whole-body barometric plethysmography (WBBP) is the most objective assessment of airflow available in conscious dogs. A BOAS index can be determined, with a higher index indicating more severe disease (on a scale of 0 to 100).This equipment is not readily available, but researchers have used it to develop BOAS functional grading to enable veterinarians to record the severity of clinical signs with improved objectivity, including changes in the condition over time or following treatment (Liu et al., 2015). Animals are graded from 0 to 3 based on the assessment of respiratory noise, inspiratory effort and dyspnoea/cyanosis/syncope before and after exercise (Table 1). Dogs with no or mild respiratory signs after exercise are considered low grade (grade 0 or 1) and may not require surgical intervention. Dogs in grades 2 or 3 would likely benefit from surgical intervention if restrictive airway malformation is present. Over time, dogs can progress into a higher grade and the history, animal’s clinical signs and owner’s perceptions can be important in deciding whether surgery might be appropriate for dogs that may soon move from a grade 1 into a grade 2.
| Respiratory noisea | Inspiratory effortb | Dyspnoea/Cyanosis/Syncopec | ||
|---|---|---|---|---|
| Grade 0 | Pre-ETT | Not audible | Not present | Not present |
| Post-ETT | Not audible | Not present | Not present | |
| Grade I | Pre-ETT | Not audible or mild | Not present | Not present |
| Post-ETT | Mild | Not present to mild | Not present | |
| Grade II | Pre-ETT | Mild to moderate | Mild to moderate | Not present |
| Post-ETT | Moderate to severe | Moderate to severe | Mild dyspnoea; cyanosis or syncope not present | |
| Grade III | Pre-ETT | Moderate to severe | Moderate to severe | Moderate to severe dyspnoea; may or may not present cyanosis. Inability to exercise |
| Post-ETT | Severe | Severe | Severe dyspnoea; may or may not present cyanosis or syncope |
Exercise intolerance
A three-minute trot has been proven to be more sensitive than a five-minute walk for the exercise testing (Riggs et al., 2019). If the dog is unable to tolerate exercise (eg osteoarthritis, obesity, anxiety) then a five-minute fast walk may be sufficient. Dogs that are stressed on presentation may approximate post-exercise assessment. Dogs previously showing syncope or cyanosis (caused by respiratory disease as opposed to cardiac or neurological conditions) are automatically grade 3, and exercise testing is therefore largely unnecessary. It is important not to force a dog to complete an exercise test if they are in respiratory difficulty or refuse exercise.
Additional tests
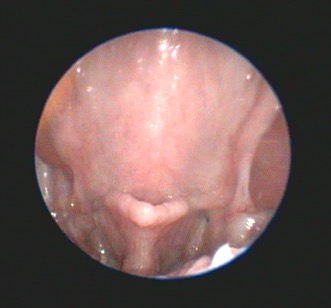
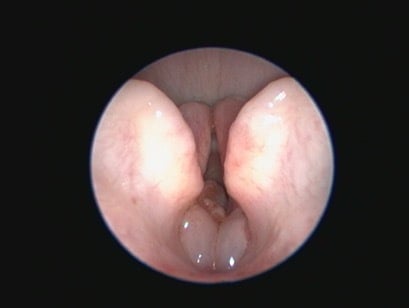
Additional diagnostic tests that can give information beyond the direct preoperative visual observation of the nostrils, soft palate (Figure 1), tonsils, laryngeal saccules (Figure 2) and laryngeal cartilages can include thoracic radiographs, computed tomography (CT) and pharyngoscopy/rhinoscopy. Findings can include aberrant nasal turbinates, aspiration pneumonia, hiatal hernia (and other oesophageal conditions), nasopharyngeal mucocoele and tracheal/bronchial disease.
Treatment
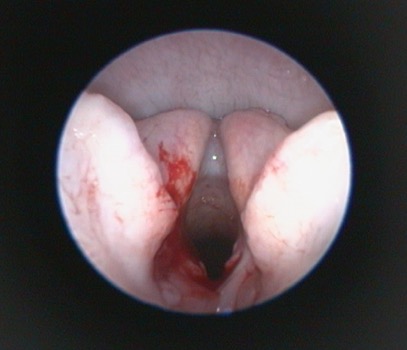
Traditional surgical treatment has largely focused on staphylectomy (soft palate resection) and rhinoplasty (nostril wedge resection). The value of laryngeal saccule excision has been debated, but overall is probably more widely performed than not (Figure 3). With increased availability of advanced imaging modalities and data from WBBP-based research, modifications of multilevel surgery (MLS) with a better outcome compared to traditional surgery include a modified folding flap palatoplasty (Figure 4), rostral alar fold resection and modified alar wing resection (Liu et al., 2017). Depending on the individual patient findings, tonsillectomy and laryngeal procedures (eg resection of everted laryngeal saccules, partial cuneiform arytenoidectomy) may also be indicated. Laser-assisted turbinectomy (LATE) can benefit some dogs, although currently in the UK this would generally be a later surgical procedure performed in refractory animals that may require some concurrent revision of the original MLS procedures. Age, body condition and laryngeal collapse have been found to be the main prognostic indicators for surgery – younger dogs, normal/underweight dogs and those with laryngeal collapse (worse than everted laryngeal saccules) have a poorer prognosis (Liu et al., 2017).

Possible risks with BOAS surgery
Besides the risks typical to general anaesthesia, airway obstruction and aspiration pneumonia must be carefully discussed with owners. Dogs with a history of regurgitation are at a higher risk of aspiration pneumonia before, during or after a general anaesthetic. The authors regularly treat heavily regurgitating dogs for 7 to 10 days preoperatively with combinations of gastroprotectant, anti-inflammatory and promotility drugs prior to airway surgery (eg sucralfate, omeprazole, prednisolone, cisapride). Thoracic auscultation and radiographs are performed prior to surgery and if pneumonia is identified, surgery may be delayed until resolution if possible (emergency presentations of BOAS or deteriorating functional grade animals may mean surgery with suboptimal timing but with clear communication with owners).
A recent study that may help practitioners quantify risk when communicating with owners applied a score to breed, surgical history, planned procedures, body condition score, level of respiratory compromise and temperature on admission – the BRisk score (Tarricone et al., 2019). These elements were found to contribute to post-operative complications following BOAS surgery. The higher the BRisk score (out of 10), the higher the risk of post-operative complications, particularly the need for oxygen support over 48 hours post-operatively, the need for a tracheostomy (either temporary or permanent) and death during hospitalisation. Dogs with a score over 3 were found to be nine times more likely to experience adverse outcomes after BOAS surgery (Tarricone et al., 2019).
Post-operative management
Post-operatively, BOAS dogs need to be closely monitored for any signs of respiratory distress. During recovery, the endotracheal tube should be removed when the dog is actively rejecting the tube and not just when the swallowing reflex is regained.
Only small amounts of soft food are fed under close supervision during the recovery period (in the authors’ practice at least four hours post-operatively, although some surgeons will starve dogs until the following morning).
Due to the risk of respiratory distress, sedatives and materials for an emergency tracheostomy should be ready at the kennel side. Perioperative intravenous steroids are often used in higher risk patients to limit airway swelling.
Nebulisation with saline can be helpful during the recovery period (in hospital and even at home) to help reduce airway inflammation and swelling, loosen any discharges and secretions which hinder breathing and improve mucous membrane health. Drugs (in particular adrenaline) can be added to nebulised saline to further minimise upper respiratory swelling (Franklin et al., 2021).
In summary
Veterinary surgeons and owners can find it challenging to determine whether brachycephalic dogs would benefit from surgical intervention for mild to moderate clinical signs. Functional grading (including an exercise test) can provide a more objective evaluation. Training and accreditation are available with the Respiratory Function Grading Scheme run with The Kennel Club and University of Cambridge. A multilevel surgical approach tailored to the findings in each individual animal is ideally performed compared to a traditional approach or one-size-fits-all approach. A detailed preoperative conversation with owners regarding risk and a mutual understanding that BOAS is never “fixed” is essential. Previously identified risk factors can help guide this discussion.
Surgeons should have a thorough understanding of the pathophysiology of the disease and the technical procedures themselves and be prepared to hospitalise and manage animals post-operatively, including familiarity with placing and caring for tracheostomy tubes. All vets, irrespective of surgical experience or interest, can apply a respiratory functional grade from a complete history and full clinical examination to dramatically improve animal assessment and guide treatment decisions.





