

Epilepsy is one of the most common chronic neurological diseases in dogs with a reported prevalence of around 0.75 percent in the total population. It is not unusual for general practitioners to be presented a pet with an episode described by the owner as vigorous jerking bodily movements. These episodes can easily be classified as an epileptiform seizure. Hallmarks of a generalised tonic-clonic seizure (GTCS) include involuntary muscle contractions and impaired consciousness along with autonomic signs during the episode such as hypersalivation, urination or defecation.
It becomes more challenging when owners present their pet with an episode of abnormal behaviour without the typical clinical manifestations of a generalised seizure. A wide range of abnormal episodes can be seen in dogs, such as facial twitching, clonus of the muscle group of one limb or behavioural changes which are not directly linked to seizure activity. These can be described as focal (previously known as partial) seizures. Many of these clinical signs can also be associated with other pathologies and the first step to diagnosis is to characterise the episode. This is easier said than done, but a better idea can be formed with the aid of owner-recorded videos and a structured step-by-step approach. In addition, it is important to realise which other conditions may mimic focal seizures and how to discriminate them.
What is a focal seizure?
Focal seizures have been defined as abnormal electrical activity arising in a localised group of neurons or networks within one hemisphere (Berendt et al., 2015). They may also progress to generalised seizures in some cases. Clinical signs depend on the brain areas involved and can be highly variable. Similarities have been found with regards to the distribution and semiology of focal seizures between dogs and humans (Berendt et al., 2004). In both, focal seizures have been associated with motor, autonomic and behavioural signs.
The literature on semiology in dogs is limited, but common motor signs are head tremors, rhythmic contractions of the facial or masticatory muscles, increased tone or clonus of one extremity and turning of the head to one side. Autonomic signs more frequently seen are lip smacking, hypersalivation and vomiting (Berendt et al., 2004; Packer et al., 2017). Abnormal behaviour is the most challenging presentation as problems in other organ systems can have a similar presentation.
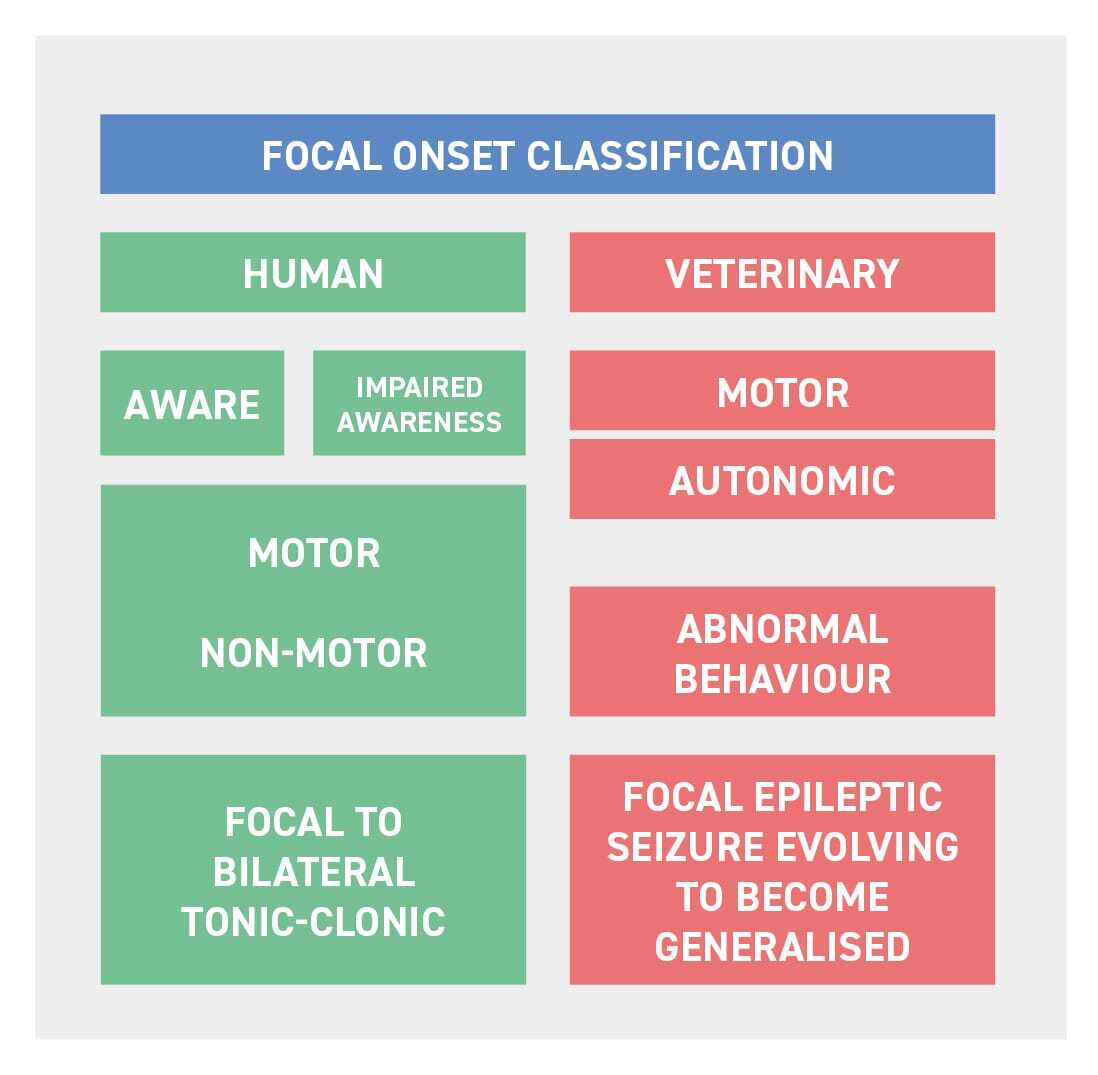
In humans, the most recent classification includes the level of awareness, motor and non-motor signs and focal to bilateral tonic-clonic seizures (Figure 1; Berendt et al., 2015). A somatosensory seizure is classified under non-motor signs and could be comparable to some of the behavioural signs seen in dogs. Abnormal skin or vision sensations may result in licking, chewing or “fly-biting”. More complex focal seizures may manifest as bizarre behaviour, such as unprovoked aggression, running uncontrollably or rhythmic barking (Berendt et al., 2004; Packer et al., 2017).
How do I know it is a focal epileptic seizure?
Recognising focal seizures relies on the owner’s report and video footage if available. Given their clinical manifestation is not as characteristic as for generalised tonic-clonic seizures, they can be difficult for an owner to detect. In addition, the perception of a focal seizure also differs compared to generalised seizures. Owners often believe a focal seizure causes less damage, is less distressing for the dog and has less impact on the quality of their dog's life, compared to generalised seizures (Packer et al., 2017). The signs appear less dramatic and owners may feel less urged to contact their veterinarian or opt for treatment. Underdiagnosis or lack of treatment may result (as with generalised seizures) in status epilepticus, which can be life-threatening and reflects the importance of recognition by both pet owner and consulting veterinarian.
The first goal is to discriminate an epileptiform seizure from any other type of “episode”. This requires a good understanding of the traits of a seizure. A few examples of these are: (1) they are often followed by a postictal period; (2) they can be associated with autonomic signs (hypersalivation, urination and defecation); and (3) they often occur directly after sleep or may be triggered by stress, noise or flashing lights.
Which other conditions should I consider?
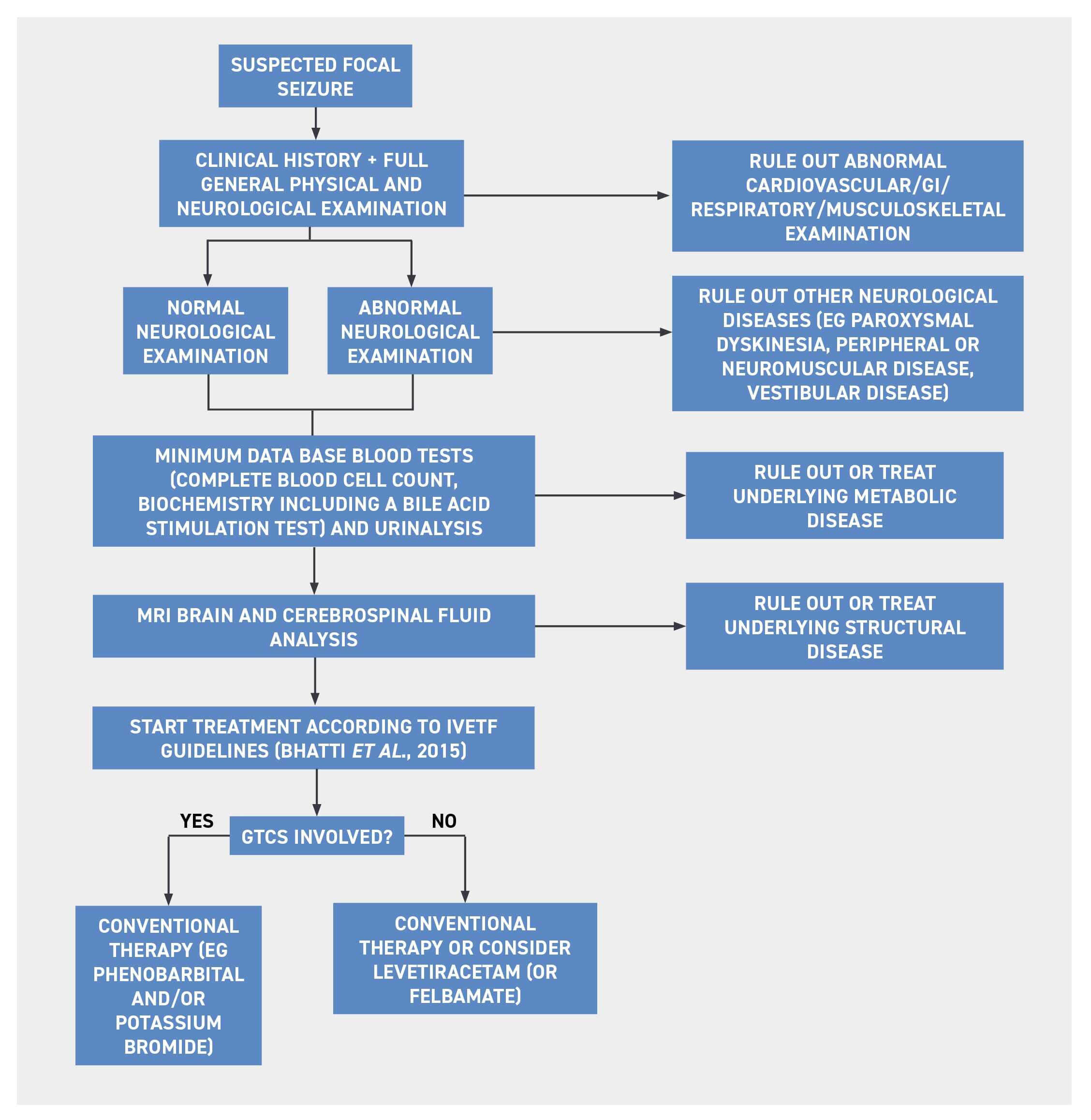
In people, the definite diagnosis of seizure activity does not solely rely upon clinical manifestation and should preferably be supported by electroencephalographical (EEG) changes (Berendt et al., 2004). EEG is unfortunately not widely available and is limited to a handful of referral centres. Therefore, we have to rely on alternative methods (Figure 2).
To help determine whether the episode is a true seizure or not, a good understanding of other conditions which may mimic focal seizures is required. One major differential diagnosis is paroxysmal dyskinesias. Paroxysmal movement disorders are a group of conditions that are characterised by episodes of abnormal movement that are self-limiting and painless, lasting from seconds to hours, with the beginning and the end of the movement disturbance being abrupt (Lowrie and Garosi, 2017b).
Other conditions which may mimic seizures include metabolic disturbances (eg hypocalcaemia, tetany), narcolepsy/cataplexy, vestibular attacks or cardiovascular collapse (syncope). Behavioural changes related to an intrinsic behavioural problem, pain, endocrine diseases or gastrointestinal diseases are also on the list of differentials. The clinical history can already get you a long way and help discriminate between types of episodes (Table 1; De Risio et al., 2015).
| DISCRIMINATOR | FOCAL SEIZURE | PAROXYSMAL DYSKINESIA |
SYNCOPE | NEUROMUSCULAR WEAKNESS |
VESTIBULAR ATTACK |
| How is the animal clinically in between the episodes? | Normal or forebrain signs | Normal | Normal or cardiovascular abnormalities | Normal or generalised weakness, muscle atrophy, decreased spinal reflexes | Normal |
| Breed predisposition? | Idiopathic epilepsy (eg Beagle, Border Collie, Bernese Mountain Dog, Golden Retriever, Labrador Retriever, Standard Poodle) Myoclonic epilepsy of unknown origin (generally in older dogs, Lafora disease: Miniature Wire-haired Dachshund, Basset Hounds, Beagles and Chihuahuas) |
Various breeds, such as: Border Terrier (canine epileptoid cramping syndrome), Cavalier King Charles Spaniel (episodic falling of CKCS), German Shorthaired Pointer (paroxysmal kinesigenic dyskinesia), Labrador Retriever and Jack Russell Terrier (paroxysmal non-kinesigenic dyskinesia) |
Chronic valvular disease: small breed dogs (eg Miniature Poodle, Cocker Spaniel, Pomeranians, Schnauzers, CKCS) Myocardial disease: large and giant breeds (eg Great Danes, Irish Wolfhounds) |
Various breeds, such as: Tibetan Mastiffs (hypertrophic neuropathy), Alaskan Malamute (polyneuropathy), Bouvier des Flandres, Siberian Huskies, Rottweilers and Bull Terriers (congenital laryngeal paralysis), Leonberger (inherited polyneuropathy) | Any, older dogs in case of idiopathic vestibular syndrome |
| Trigger? | None or flashing lights, anxiety, stress | None or activity, exercise, excitement, stress | Exercise, excitement | Activity, exercise | None |
| How long does the episode last? | Seconds to minutes or more than 5 min in case of status epilepticus | Seconds to hours | Seconds | Minutes to hours | Seconds to hours |
| Is the animal conscious? | Often conscious but both unconscious and conscious are possible | Conscious even in cases involving all four limbs | Reduced to absent | Normal | Normal or disorientated |
| Pre-episodic changes? | Pre-ictal signs may include anxiety, restlessness, increased affection, contact-seeking, withdrawal, hiding, aggressiveness and vocalisation | None | None | None | None |
| Post-episodic changes? | Post-ictal signs may include disorientation, aggressive behaviour, restlessness, pacing, lethargy, deep sleep, hunger, thirst and ataxia | None or tiredness | None | None | None |
| Is the episode associated with autonomic signs? | Hypersalivation, defecation and urination present in 23 to 48.1 percent of cases | No | Possible cardiovascular abnormalities | No | No |
| Muscle tone? | Normal to increased | Hypertonicity (focal or generalised) | Flaccid (whole body) | Often flaccid | Unilateral decrease in extensor muscle |
| Do the episodes respond to anticonvulsant treatment? | Possible | No | No | No | No |
| Does the animal also have GTCS? | Often | No | No | No | No |
| Other | Interaction with the owner does not interrupt the episode | Interaction with the owner can alleviate or interrupt the episode | May be accompanied by cough, increased respiratory noise | May be accompanied by dysphagia, dysphonia, regurgitation, dyspnoea | Subtle signs of vestibular disease might persist |
Epilepsy and paroxysmal dyskinesia are more often idiopathic, but both can have underlying metabolic or structural brain pathology. These causes should ideally be ruled out before treating a dog for idiopathic epilepsy. A trial therapy can be considered in cases with a normal physical examination and after ruling out metabolic diseases, should referral be declined.
When do I start treatment for focal seizures and which one should I use?
An important thing to note is that a focal seizure is a clinical sign and not a diagnosis. Focal seizures can be primary or secondary and if an underlying brain disease or metabolic disease has been identified, this should be treated concurrently. Although focal seizures may not look as dramatic, underestimation may potentially jeopardise the patient’s quality of life (QoL). Deciding when to start treatment does not differ greatly compared to cases with GTCS and the guidelines according to the International Veterinary Epilepsy Task Force (IVETF), which are available online for free, should be consulted (Bhatti et al., 2015).
As with most forms of epileptic seizure activity, anti-convulsant medications are the cornerstone of therapy. With focal seizures there is, however, limited information available about the benefits of conventional therapy such as phenobarbital and potassium bromide, regardless of the underlying pathology. The only anticonvulsant medication specifically aimed at focal seizures and shown to reduce seizure frequency is felbamate. However, this has only been tested on a small number of dogs (Ruehlmann et al., 2001).
A few studies have focused on treatment of myoclonic seizures. Although success appears to be limited, some beneficial response has been seen with the use of levetiracetam (Lowrie and Garosi, 2017a). Having said that, phenobarbital, potassium bromide or imepitoin are still the first choice when GTCS are also involved which is often the case. Although the presentation can be highly variable, as with GTCS the aim of managing epileptic patients with focal seizures is to limit the frequency and intensity of seizures whilst producing minimal side effects.
Focal seizures can be very challenging to detect as they may mimic many other conditions and they may be underdiagnosed given they are less distressful for the owner compared to GTCS. However, early recognition and treatment is important to prevent further evolvement to GTCS and status epilepticus, which can be life-threatening. Anti-convulsant medications are the cornerstone of therapy; however, studies on treatment for focal seizures are limited and trial treatment with several drugs may be required. We hope this report helps the clinician to take the first steps in successfully managing focal seizures by discriminating them from other conditions in order to develop an appropriate treatment plan.
_FF_CourseThumb.jpg?width=500&height=300&name=IVE_GPCert(Neuro)_FF_CourseThumb.jpg)
Small Animal Neurology
ISVPS General Practitioner Certificate (GPCert)
 July 2026
July 2026
 Online
Online
References (click to expand)
| Berendt, M., Gredal, H. and Alving, J. | 2004 | Characteristics and phenomenology of epileptic partial seizures in dogs: similarities with human seizure semiology. Epilepsy Research, 61, 167-173 |
| Berendt, M., Farquhar, R., Mandigers, P., Pakozdy, A., Bhatti, S., De Risio, L., Fischer, A., Long, S., Matiasek, K., Muñana, K., Patterson, E., Penderis, J., Platt, S., Podell, M., Potschka, H., Pumarola, M., Rusbridge, C., Stein, V., Tipold, A. and Volk, H. | 2015 | International Veterinary Epilepsy Task Force consensus report on epilepsy definition, classification and terminology in companion animals. BMC Veterinary Research, 11 |
| Bhatti, S., De Risio, L., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farquhar, R., Fischer, A., Long, S., Löscher, W., Mandigers, P., Matiasek, K., Pakozdy, A., Patterson, E., Platt, S., Podell, M., Potschka, H., Rusbridge, C. and Volk, H. | 2015 | International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Veterinary Research, 11 |
| De Risio, L., Bhatti, S., Muñana, K., Penderis, J., Stein, V., Tipold, A., Berendt, M., Farqhuar, R., Fischer, A., Long, S., Mandigers, P., Matiasek, K., Packer, R., Pakozdy, A., Patterson, N., Platt, S., Podell, M., Potschka, H., Batlle, M., Rusbridge, C. and Volk, H. | 2015 | International Veterinary Epilepsy Task Force consensus proposal: diagnostic approach to epilepsy in dogs. BMC Veterinary Research, 11 |
| Lowrie, M. and Garosi, L. | 2017a | Classification of involuntary movements in dogs: myoclonus and myotonia. Journal of Veterinary Internal Medicine, 31, 979-987 |
| Lowrie, M. and Garosi, L. | 2017b | Classification of involuntary movements in dogs: paroxysmal dyskinesias. The Veterinary Journal, 220, 65-71 |
| Packer, R., Lucas, R. and Volk, H. | 2017 | BSAVA Manual of Canine and Feline Neurology, 4th ed. BSAVA, Gloucester |
| Ruehlmann, D., Podell, M. and March, P. | 2001 | Treatment of partial seizures and seizure-like activity with felbamate in six dogs. Journal of Small Animal Practice, 42, 403-408 |






